

Childhood Speech problems (Apraxia)
What is childhood apraxia of speech?
Childhood apraxia of speech (CAS) is a motor speech disorder. Children with CAS have problems saying sounds, syllables, and words. This is not because of muscle weakness or paralysis. The brain has problems planning to move the body parts (e.g., lips, jaw, tongue) needed for speech. The child knows what he or she wants to say, but his/her brain has difficulty coordinating the muscle movements necessary to say those words.
What are some signs or symptoms of childhood apraxia of speech?
 Not all children with CAS are the same. All of the signs and symptoms listed below may not be present in every child. It is important to have your child evaluated by a speech-language pathologist (SLP) who has knowledge of CAS to rule out other causes of speech problems. General things to look for include the following:
Not all children with CAS are the same. All of the signs and symptoms listed below may not be present in every child. It is important to have your child evaluated by a speech-language pathologist (SLP) who has knowledge of CAS to rule out other causes of speech problems. General things to look for include the following:
A Very Young Child
- Does not coo or babble as an infant
- First words are late, and they may be missing sounds
- Only a few different consonant and vowel sounds
- Problems combining sounds; may show long pauses between sounds
- Simplifies words by replacing difficult sounds with easier ones or by deleting difficult sounds (although all children do this, the child with apraxia of speech does so more often)
- May have problems eating
An Older Child
- Makes inconsistent sound errors that are not the result of immaturity
- Can understand language much better than he or she can talk
- Has difficulty imitating speech, but imitated speech is more clear than spontaneous speech
- May appear to be groping when attempting to produce sounds or to coordinate the lips, tongue, and jaw for purposeful movement
- Has more difficulty saying longer words or phrases clearly than shorter ones
- Appears to have more difficulty when he or she is anxious
- Is hard to understand, especially for an unfamiliar listener
- Sounds choppy, monotonous, or stresses the wrong syllable or word
Potential Other Problems
- Delayed language development
- Other expressive language problems like word order confusions and word recall
- Difficulties with fine motor movement/coordination
- Over sensitive (hypersensitive) or under sensitive (hyposensitive) in their mouths (e.g., may not like toothbrushing or crunchy foods, may not be able to identify an object in their mouth through touch)
- Children with CAS or other speech problems may have problems when learning to read, spell, and write
How is childhood apraxia of speech diagnosed?
An audiologist should perform a hearing evaluation to rule out hearing loss as a possible cause of the child’s speech difficulties.
A certified-SLP with knowledge and experience with CAS conducts an evaluation. This will assess the child’s oral-motor abilities, melody of speech, and speech sound development. The SLP can diagnose CAS and rule out other speech disorders, unless only a limited speech sample can be obtained making a firm diagnosis challenging.
An oral-motor assessment involves:
- checking for signs of weakness or low muscle tone in the lips, jaw, and tongue, called dysarthria. Children with CAS do not usually have weakness, but checking for weakness will help the SLP make a diagnosis.
- seeing how well the child can coordinate the movement of the mouth by having him or her imitate nonspeech actions (e.g., moving the tongue from side to side, smiling, frowning, puckering the lips)
- evaluating the coordination and sequencing of muscle movements for speech while the child performs tasks such as the diadochokinetic rate, which requires the child to repeat strings of sounds (e.g., puh-tuh-kuh) as fast as possible
- examining rote abilities by testing the child’s skills in functional or “real-life” situations (e.g., licking a lollipop) and comparing this to skills in nonfunctional or “pretend” situations (e.g., pretending to lick a lollipop)
A melody of speech (intonation) assessment involves:
- listening to the child to make sure that he or she is able to appropriately stress syllables in words and words in sentences
- determining whether the child can use pitch and pauses to mark different types of sentences (e.g., questions vs. statements) and to mark off different portions of the sentence (e.g., to pause between phrases, not in the middle of them)
A speech sound (pronunciation of sounds in words) assessment involves:
- Evaluating both vowel and consonant sounds
- Checking how well the child says individual sounds and sound combinations (syllables and word shapes)
- Determining how well others can understand the child when they use single words, phrases, and conversational speech.
An SLP may also examine the child’s receptive and expressive language skills and literacy skills to see if there are co-existing problems in these areas.
What treatments are available for children with apraxia of speech?
 Research shows the children with CAS have more success when they receive frequent (3-5 times per week) and intensive treatment. Children seen alone for treatment tend to do better than children seen in groups. As the child improves, they may need treatment less often, and group therapy may be a better alternative.
Research shows the children with CAS have more success when they receive frequent (3-5 times per week) and intensive treatment. Children seen alone for treatment tend to do better than children seen in groups. As the child improves, they may need treatment less often, and group therapy may be a better alternative.
The focus of intervention for CAS is on improving the planning, sequencing, and coordination of muscle movements for speech production. Isolated exercises designed to “strengthen” the oral muscles will not help with speech. CAS is a disorder of speech coordination, not strength.
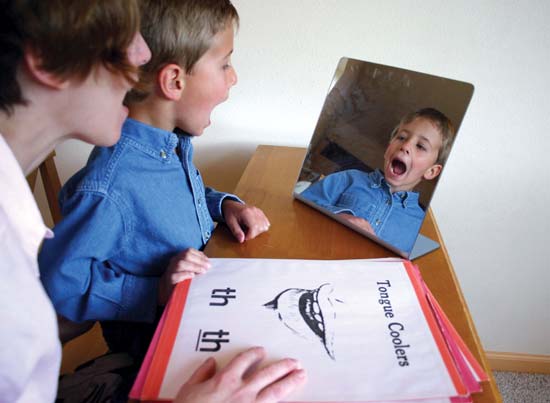
To improve speech, the child must practice speech. However, getting feedback from a number of senses, such as tactile “touch” cues and visual cues (e.g., watching him/herself in the mirror) as well as auditory feedback, is often helpful. With this multi-sensory feedback, the child can more readily repeat syllables, words, sentences and longer utterances to improve muscle coordination and sequencing for speech.
Some clients may be taught to use sign language or an augmentative and alternative communication system (e.g., a portable computer that writes and/or produces speech) if the apraxia makes speaking very difficult. Once speech production is improved, the need for these systems may lessen, but they can be used to support speech or move the child more quickly to higher levels of language complexity.
Practice at home is very important. Families will often be given assignments to help the child progress and allow the child to use new strategies outside of the treatment room, and to assure optimal progress in therapy.
One of the most important things for the family to remember is that treatment of apraxia of speech takes time and commitment. Children with CAS need a supportive environment that helps them feel successful with communication. For children who also receive other services, such as physical or occupational therapy, families and professionals need to schedule services in a way that does not make the child too tired and unable to make the best use of therapy time.
To contact a speech-language pathologist, visit ASHA’s Find a Professional.
What other organizations have information about childhood apraxia of speech?
This list is not exhaustive and inclusion does not imply endorsement of the organization or the content of the Web site by ASHA.
- Apraxia-Kids information site
- National Institute on Deafness and Other Communication Disorders
- Speechville Express
What causes childhood apraxia of speech?
 Childhood apraxia of speech (CAS) is a motor speech disorder. There is something in the child’s brain that is not allowing messages to get to the mouth muscles to produce speech correctly. In most cases, the cause is unknown. However, some possible causes include:
Childhood apraxia of speech (CAS) is a motor speech disorder. There is something in the child’s brain that is not allowing messages to get to the mouth muscles to produce speech correctly. In most cases, the cause is unknown. However, some possible causes include:
- Genetic disorders or syndromes
- Stroke or brain injury
It is important to note that while CAS may be referred to as “developmental apraxia,” it is not a disorder that children simply “outgrow.” For many developmental speech disorders, children learn sounds in a typical order, just at a slower pace. In CAS, children do not follow typical patterns and will not make progress without treatment. There is no cure, but with appropriate, intensive intervention, significant progress can be made.
How common is childhood apraxia of speech?
There is little data available about how many children have CAS. The number of children diagnosed with CAS appears to be on the rise, but it is hard to know how the incidence has changed over time. Some factors influencing this rise include:
- Increased awareness of CAS by professionals and families
- Increased availability of research on CAS
- Earlier-age evaluation and identification
What do speech-language pathologists do when working with children with apraxia of speech?
ASHA published two documents on CAS that outline the role of the SLP in the evaluation, diagnosis, and treatment of children with the disorder.
The Preferred Practice Patterns for the Profession of Speech-Language Pathology outline the common practices followed by SLPs when engaging in various aspects of the profession.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment